If You (Re)Build It, Will They Come? Evidence from California
Presenter: Zach Levin, Federal Trade Commission Discussant: Ian McCarthy, Emory University and NBER
MHEC, September 7, 2023
Background
Research Question
What happens after construction of a new hospital?
- Utilization at focal hospital versus other hospitals in the market
- Quality changes, clinical and non-clinical
Relevant Literatures
- Entry and competition in hospital markets
- Patient preferences for clinical quality versus amenities
- Non-profit hospitals and incentives for overuse?
1. Entry and Competition
- Mid 1960s: Increasing concern about hospital costs and excess capacity, duplicative services and facilities
- 1964: New York State enacts the first certificate of need (CON) program
- 1974: National Health Planning and Resources Development Act requires all states to have CON programs
- 1980: CON laws in place for all states except Louisiana
Enacted during cost-plus reimbursement, where hospitals had little incentive to control costs
1. Entry and Competition
- 1986: Congress repeals the National Health Planning and Resources Development Act
- 1990s: Many states repeal or weaken CON laws
- Today: 35 states and the District of Columbia still have some form of CON laws, 14 states have CON laws that apply specifically to hospitals
As a binding barrier to entry, CON often cited as part of the hospital pricing problem
2. Patient Preferences
- Strong evidence that patients value non-clinical quality
- Construction implies shiny new buildings, private rooms, etc.
3. Non-profit Hospitals
- Possible to link construction with NFP status?
- Reinvesting profits back into system (as necessary for NFP status) may over-incentivize construction
- Policy implications re NFP status if such construction is “wasteful”
- Potential call for more oversight of tax benefits
What does this paper do?
Basic Idea
- 2006: California enacts SB 1953, requiring all hospitals to meet seismic safety standards by 2030
- 90% of hospitals did not meet these standards in 2006
- 2009-2015: 41 non-ED expansions or rebuilds
Empirical Strategy
Stacked difference-in-differences
- Treatment: hospital in California that expands or rebuilds in 2009-2015
- Control: hospitals in other markets (20+ miles away) that do not expand or rebuild
- Time: pre- and post-construction
Findings
- Construction projects yield 10%+ increase in admissions
- Patients more likely to recommend hospitals after construction
- No evidence of changes in clinical quality
Some Conceptual Questions
Implications for CON Laws?
- In what ways are CON laws binding?
- Own-hospital expansion? (seems unlikely)
- Entry by new hospitals? (seems more likely)
Implications for Amenities?
- Large capital investments imply investment in amenities
- Can this be measured directly?
- Is “room always quite” or “always respond quickly” an amenity?
Some Empirical Questions
Why did the hospitals expand or rebuild?
…though I am unable to differentiate whether this growth is a response to unmet needs.
Things to consider:
- Pre-construction occupancy to identify capacity constrained vs. unconstrained hospitals (by admission category)
- Admission or procedure codes before/after construction to identify services that expanded
Treated vs. Control
- Treated hospitals appear very different than control hospitals
- Bigger, higher occupancy, less Medicaid, less for-profit, more teaching hospitals
Things to consider:
- Reweighting on pre-expansion size, occupancy, etc.
- Not-yet-treated as controls in stacked setup
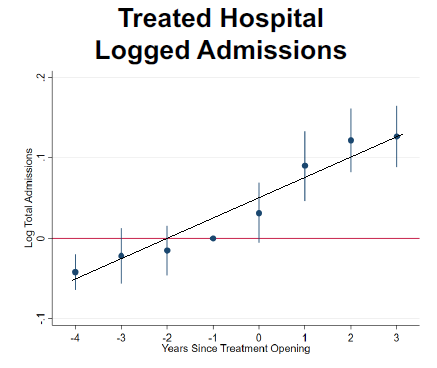
Pre-trends/confounding
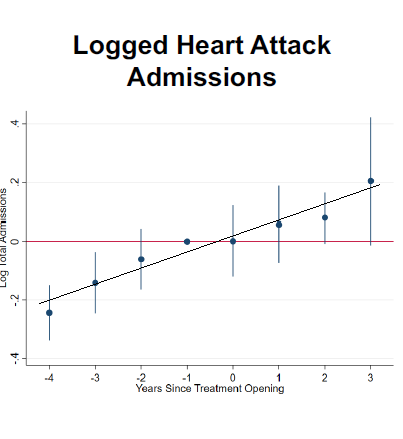
Pre-trends/confounding
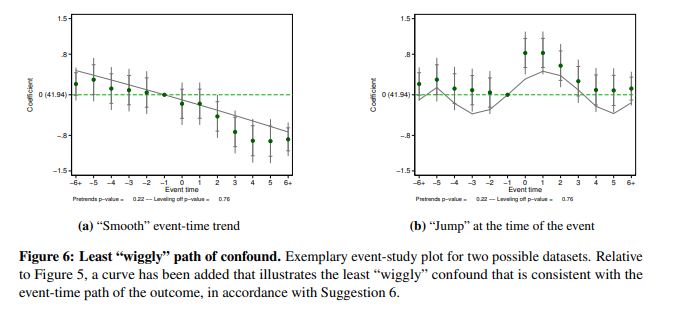
Potential Solution
Final Thoughts
My Takeaways
- Great data, well suited to study effects of hospital construction
- Decomposing additional admissions into expansion versus unmet need is important here
- Consider reframing on NFP status and policies rather than CON laws or amenities
Thank You!
Ian McCarthy, Emory University & NBER
ianmcccarthyecon.com
ian.mccarthy@emory.edu