Origin of Physician Practice Variation: Role of Training and Clinical Trials
Presenter: Bingxiao Wu, Rutgers University
Discussant: Ian McCarthy, Emory University and NBER
Discussant: Ian McCarthy, Emory University and NBER
ASHEcon, June 12, 2023
Background
Geographic Variation in Health Care Spending
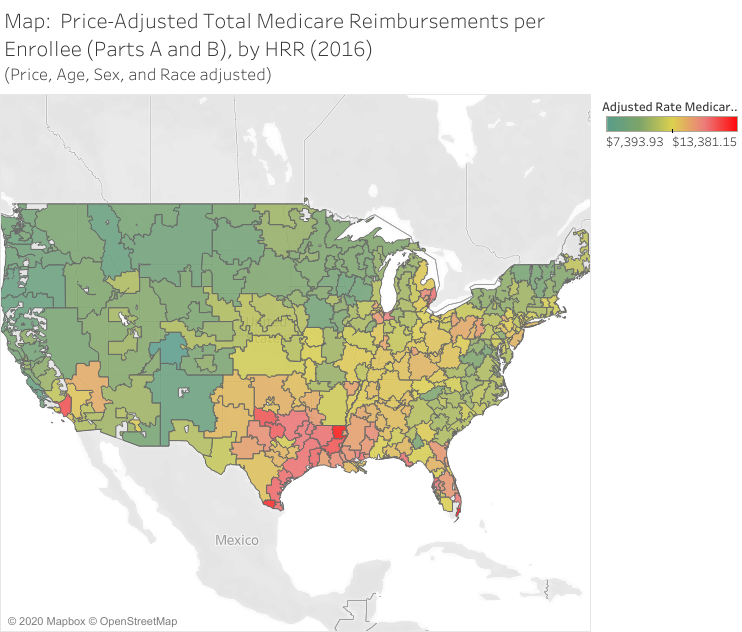
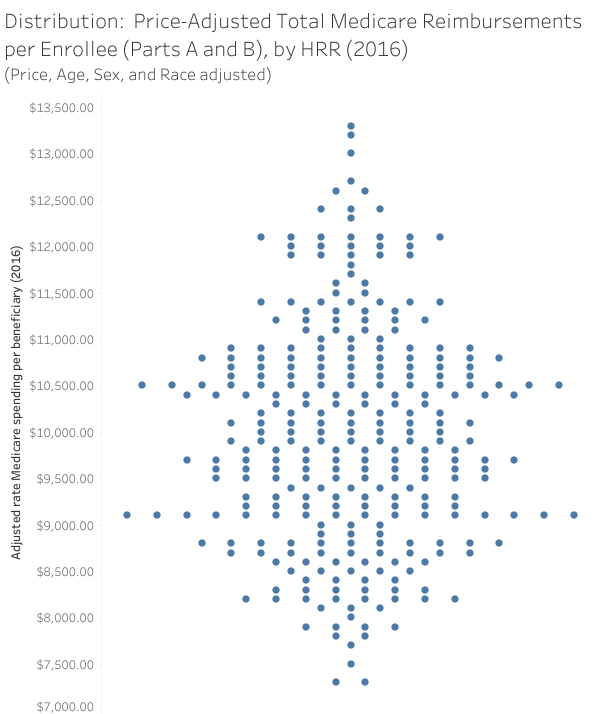
Variation is not just in spending across geographic areas…also exists:
- quality of care
- within geographic markets
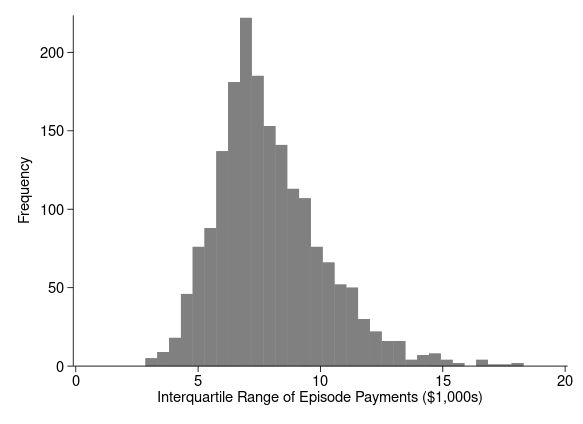
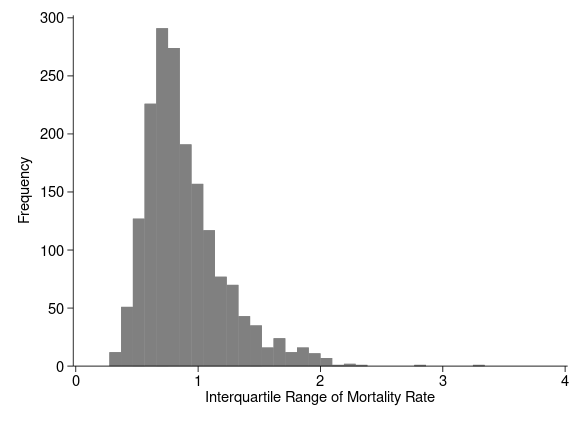
Within-market Variation in Health Care Spending and Quality
Research Question
Does a physician’s training explain some amount of the observed variation in care?
What does this paper do?
Empirical strategy
- Transcatheter Aortic Valve Replacement (TAVR)
- Exploit launch of PARTNER TAVR trials in 22 hospitals in 2007
- “trained” physicians compared to “matched” physicians with same fellowship location but just before PARTNER trial
Empirical strategy
- Compare physicians with and without PARTNER training
- Compare physicians exposed to a trained physician versus not (spillovers)
Findings
- Trained physicians much more likely to use TAVR
- 150% more likely to use TAVR when part of PARTNER trial
- Untrained physicians “around” trained physicians also more likely to use TAVR
- 12% more TAVR when practicing in the same zip code as a trained physician
Some thoughts
Minor interpretation question
- Is “1.5 times more likely” the right conclusion?
- Or should it be 1.5 times faster?
- Estimates on volume are much smaller (between 20% and 35%)
Metrics point
- Some growing skepticism with \(ln(y + \text{c})\) (Mullahy and Norton, 2023)
- Consider OLS on untransformed outcome, two-part model, or Poisson
TAVR adoption is pretty complicated
- TAVR first approved only for high-risk patients ineligible for SAVR
- Later approved for SAVR-eligible high-risk and eventually intermediate risk
- Hospital infrastructure requirements
- Hospital and physician volume requirements
TAVR adoption is pretty complicated
- Requires hospital commitment and likely direct investment
- Availability depends on physician’s prior experience
- Are results a reflection of physician skill/preference or…
- hospital willingness/ability to invest in TAVR program
- physician switching costs due to differential volume requirements with prior TAVR experience
Suggestions moving forward
- Incorporate volume and infrastructure requirements when constructing matched pairs
- Want to make sure hospitals are on equal footing
Takeaways
- How do we explain observed variation? Great question with clear policy implications
- Good identification strategy to test role of clinical training
- Complicated setting but seems doable given data
Thank You!
Ian McCarthy, Emory University & NBER
ianmcccarthyecon.com
ian.mccarthy@emory.edu